GLP-1 Medications and Gallbladder Disease: A Surgeon's Guide
GLP-1 medications like Mounjaro, Wegovy and Ozempic are transforming weight management — but peer-reviewed evidence shows they substantially increase the risk of gallbladder problems. This page explains why, who is most affected, the symptoms to recognise, and when a surgical assessment is appropriate.
I am a consultant surgeon at the Wessex Nuffield in Southampton and in the NHS. I assess and treat patients who’ve developed gallbladder problems on GLP-1 medications, usually within a week. I welcome patients who have decided on surgery, or if you simply want to understand your risk before it becomes a problem.
Why GLP-1 medications affect the gallbladder
GLP-1 receptor agonists are highly effective for weight management and glycaemic control. They also have two effects on the biliary system that, together, substantially increase the risk of gallstone disease:
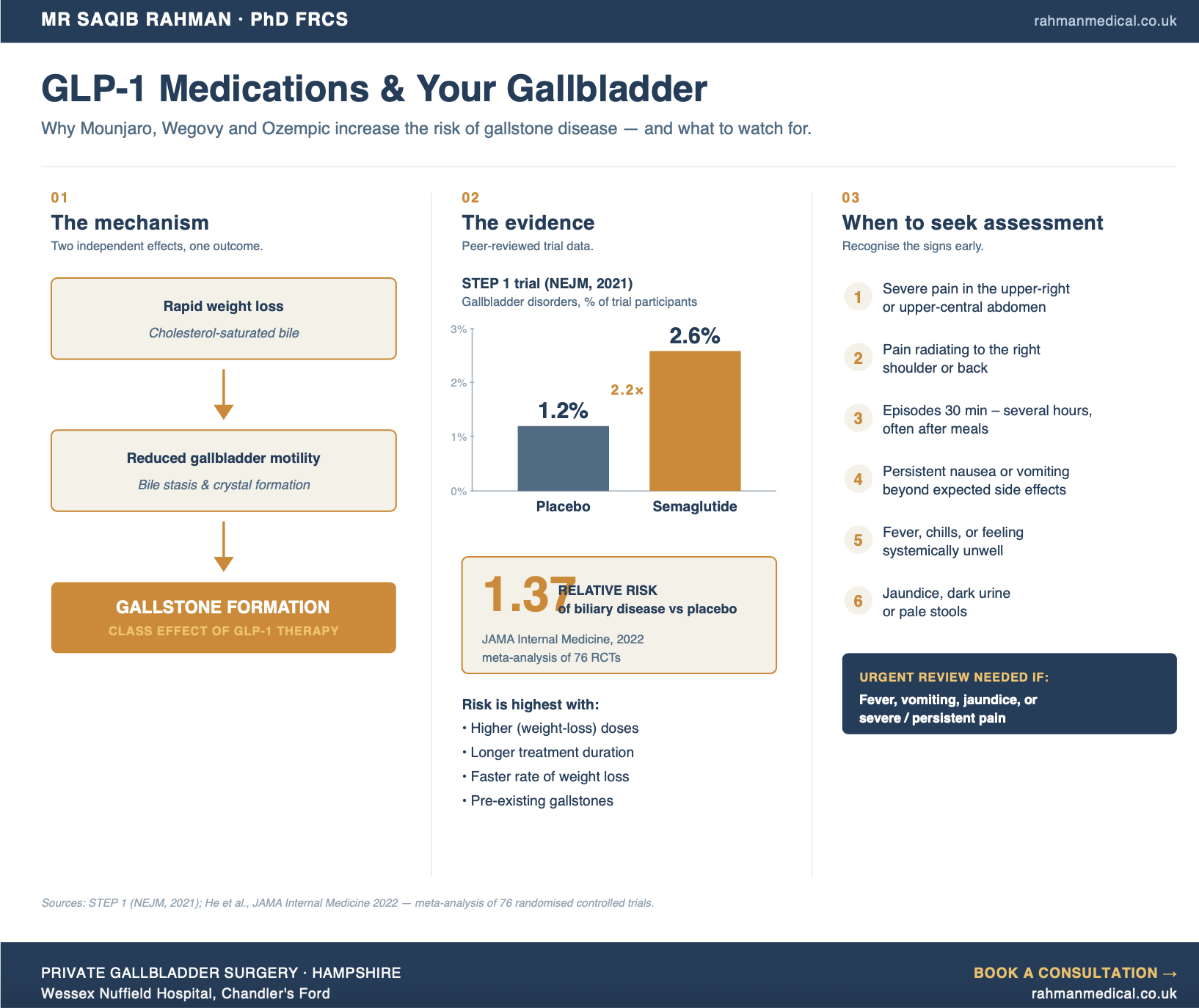
• Rapid weight loss alters bile composition. As body fat reduces quickly, cholesterol concentration in bile rises. Supersaturated bile is the precursor to cholesterol gallstone formation. The faster the weight loss, the higher the risk.
• Reduced gallbladder motility. GLP-1s slow gastric emptying, and this effect extends to the gallbladder. Reduced contraction frequency means bile sits for longer in the gallbladder — a state called bile stasis — giving cholesterol crystals the time and conditions to coalesce into solid stones.
These two mechanisms are independent and additive. Together they explain why biliary disease is a recognised class effect of GLP-1 therapy.
What the clinical evidence shows
Several large, peer-reviewed studies have quantified the risk:
• The STEP 1 trial (NEJM, 2021): patients on high-dose semaglutide lost an average of 14.9% of their body weight over 68 weeks. Gallbladder disorders were reported in 2.6% of patients on semaglutide versus 1.2% on placebo — more than double the rate.
• 2022 JAMA Internal Medicine meta-analysis: pooling 76 randomised controlled trials, GLP-1 receptor agonist use was associated with a relative risk of 1.37 for biliary disease compared with placebo or other treatments. The association was strongest at weight-loss dosages and with longer treatment duration.
• Acute cholecystitis (gallbladder infection) and biliary colic are the most common presentations. Gallstone pancreatitis and obstructive jaundice are rarer but more serious.
The absolute risk per patient remains modest, but the very large and growing number of people on these medications means the absolute number of patients presenting with biliary complications is substantial — and rising.
Who is most at risk?
The evidence consistently identifies several factors that increase risk further:
• Higher doses (the weight-loss doses of semaglutide and tirzepatide carry higher risk than the lower diabetic doses)
• Longer duration of treatment
• Faster rate of weight loss
• Pre-existing gallstones — even asymptomatic ones found on a previous scan
• Female sex, age over 40, and family history of gallstones (the standard baseline risk factors, amplified by GLP-1 therapy)
If several of these apply to you, the risk-benefit balance of your treatment plan is worth a structured discussion.
Symptoms to watch for
Gallbladder symptoms while on GLP-1 therapy can be missed because some overlap with the side effects of the medication itself (nausea, abdominal discomfort). The features that should prompt assessment are:
• Severe, sudden pain in the upper right or upper central abdomen
• Pain radiating to the right shoulder or to the centre of the back
• Pain that comes in episodes lasting 30 minutes to several hours, particularly after meals
• Persistent nausea or vomiting beyond the expected GLP-1 side-effect window
• Fever, chills, or feeling systemically unwell
• Yellowing of the skin or eyes (jaundice)
• Dark urine or pale stools
The last three suggest more serious complications and warrant urgent medical review.
If you already have asymptomatic gallstones and are starting GLP-1 therapy
This is one of the highest-risk situations and one of the most under-discussed. A patient with previously incidental gallstones who starts high-dose GLP-1 therapy has a substantially elevated risk of developing an acute biliary event. For these patients, an individualised risk assessment before or shortly after starting treatment is worthwhile. We use the RELAPSTONE risk-assessment tool, derived from peer-reviewed clinical trial data, to estimate your specific probability of developing symptoms — allowing a properly informed decision about whether to consider elective cholecystectomy before symptoms occur. For a fuller discussion of the asymptomatic gallstone question, see our dedicated page on asymptomatic gallstones.
If you develop new gallbladder symptoms on GLP-1 therapy
If biliary symptoms have started since beginning treatment, the diagnostic pathway is:
• Clinical history and examination
• Abdominal ultrasound — the definitive imaging for gallstones
• Blood tests including liver function and inflammatory markers
• In selected cases, MRCP (a specialised MRI of the bile ducts)
Once gallstones are confirmed, the question becomes whether to proceed with cholecystectomy. For most symptomatic patients the evidence-based answer is yes, because symptoms tend to recur and complications carry significant morbidity. The RELAPSTONE tool quantifies your individual probability of recurrence without surgery, which makes the decision more concrete than a general statistic.
Can I continue GLP-1 therapy if I develop gallstones?
In most cases, yes. There is no absolute contraindication to continuing treatment after diagnosis, but the clinical picture matters:
• Asymptomatic gallstones found incidentally: discussion of risk versus benefit; many patients continue treatment with monitoring
• Single episode of biliary colic: usually an indication for cholecystectomy, after which GLP-1 therapy can typically continue uninterrupted
• Acute cholecystitis or other complication: urgent surgical management, with GLP-1 therapy paused and reintroduced after recovery
The decision is individualised and made jointly with your prescribing clinician.
Is pre-emptive surgery ever recommended?
For patients without pre-existing gallstones, no — the evidence does not support routine prophylactic cholecystectomy before starting GLP-1 therapy. The majority of patients will not develop biliary disease, and the risks of unnecessary surgery outweigh the population-level benefit. For patients with known asymptomatic gallstones who are about to start high-dose GLP-1 therapy, the balance is different and pre-emptive surgery may be reasonable. This decision benefits from a formal surgical assessment with individualised risk estimation.
What an assessment involves
A typical consultation includes:
• A focused history of your GLP-1 treatment (medication, dose, duration, rate of weight loss)
• Review of any symptoms, including subtle or partial ones
• Examination
• Review of any existing imaging
• Discussion of your individual risk profile, with the RELAPSTONE tool where
appropriate
• A clear summary of the options, with no pressure to proceed
If imaging is needed, this can be arranged. If surgery is the right decision, laparoscopic cholecystectomy is performed as a day case at the Wessex Nuffield Hospital. For an overview of the procedure, see our dedicated page.
Common questions about GLP-1 and gallbladder disease
1
Are some GLP-1 medications safer for the gallbladder than others?
All GLP-1 receptor agonists studied — semaglutide (Wegovy, Ozempic), tirzepatide (Mounjaro), liraglutide (Saxenda, Victoza) — show the same class effect on biliary disease. The risk correlates more strongly with dose and rate of weight loss than with the specific molecule.
Will I definitely get gallstones if I take Mounjaro or Wegovy?
2
No. The absolute risk for any individual patient remains modest — around 2–3% in trial populations. Most people on these medications never develop biliary disease. The point is to recognise that the risk is elevated and to respond appropriately if symptoms appear.
Should I have an ultrasound before starting GLP-1 therapy?
3
Routine screening ultrasound for everyone starting treatment is not currently standard practice. However, if you have a family history of gallstones, previous biliary symptoms, or other risk factors, a baseline ultrasound can be reasonable and would inform decisions later if symptoms develop.
I've already lost the weight I wanted to. Does the gallbladder risk go away once I stop the medication?
4
The peak risk window is during active weight loss. Once weight stabilises and the medication is discontinued, the additional GLP-1-driven risk diminishes. However, any gallstones that have formed during treatment remain and can cause symptoms at any future point.
My GP has prescribed Mounjaro and I've had right-sided pain. What should I do?
5
New upper-right or upper-central abdominal pain in a patient on GLP-1 therapy warrants assessment — not because it is always gallstones, but because the prior probability is higher than in the general population. Acute, severe, or persistent pain, or any pain with fever, vomiting or jaundice, needs urgent review.
New gallbladder symptoms on a GLP-1 medication are worth getting assessed promptly. I can usually see you within a week — bring any existing scans and we'll get you a clear answer.
Next steps
If you are on a GLP-1 medication and have developed gallbladder symptoms, or have known gallstones and want a specialist opinion before continuing treatment:
This page is part of our gallbladder information resource. See also our guide to private gallbladder surgery in Southampton and asymptomatic gallstones page.