Do I Need Surgery for Gallstones without symptoms?
A Surgeons Guide
Many patients are told they have gallstones after an ultrasound for an unrelated problem. The diagnosis raises an immediate question: do I need surgery, or can this be safely left alone? The honest answer is "it depends" — and this page explains exactly what it depends on.
I am a consultant surgeon at the Wessex Nuffield Hospital in Southampton and the NHS. I see patients usually within a week, including for second opinions on whether surgery is needed at all.
How common are asymptomatic gallstones?
Gallstones are present in around 10–15% of UK adults. The majority of these patients have no symptoms at all and the stones are discovered incidentally — typically on an abdominal ultrasound scan performed for another reason. This situation is called asymptomatic cholelithiasis. Finding gallstones on a scan does not, by itself, mean surgery is necessary.
What does the evidence say about progression?
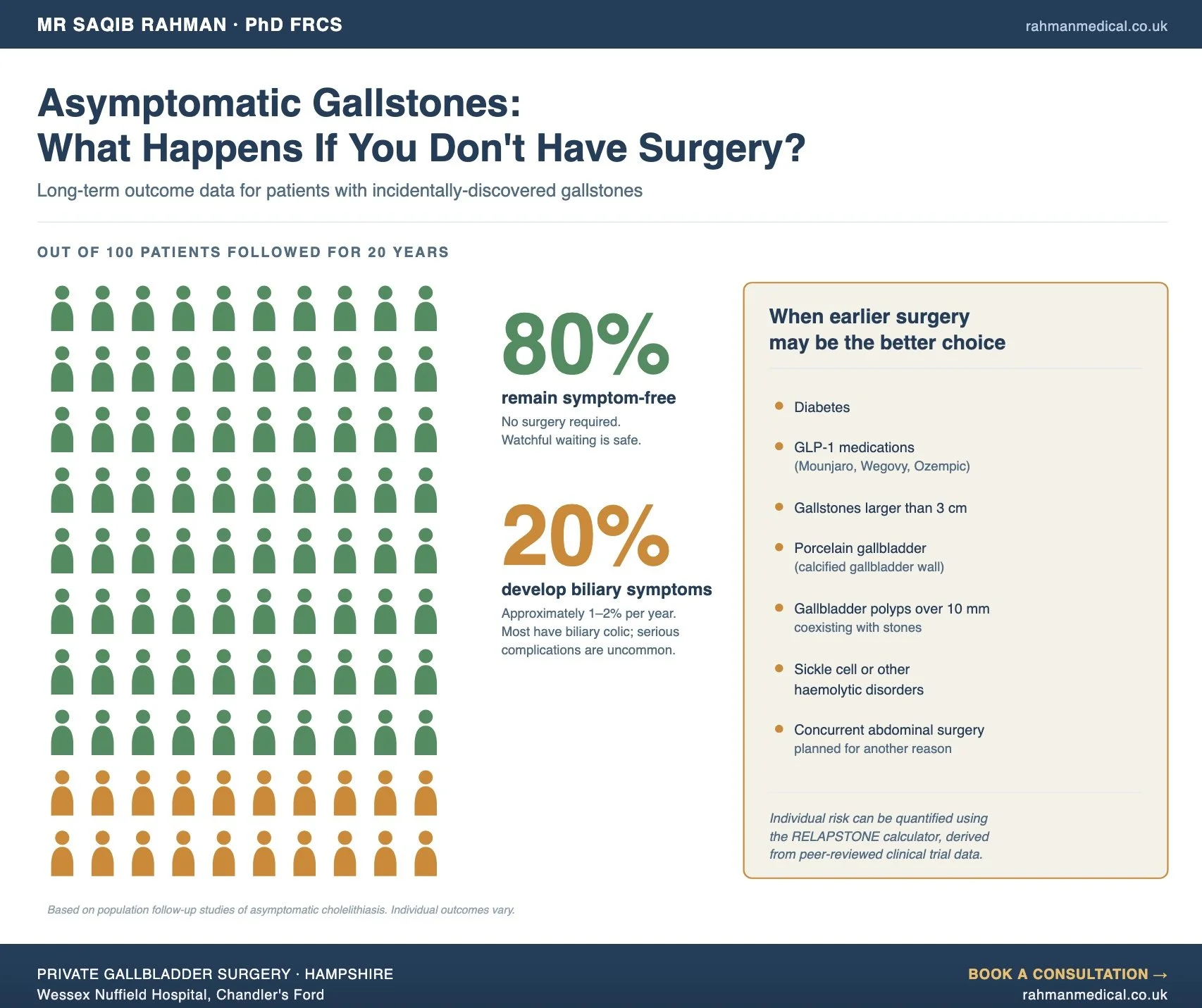
The most consistent finding across decades of follow-up studies is that the majority of patients with asymptomatic gallstones remain symptom-free. Approximately 1–2% per year will develop biliary symptoms, with a cumulative rate of around 20% over 20 years. The remaining 80% never develop a problem that requires intervention. Of those who do develop symptoms, most have biliary colic — episodes of severe upper abdominal pain — rather than serious complications. Around 1–3% per year of symptomatic patients go on to develop more serious problems such as acute cholecystitis, gallstone pancreatitis, or obstructive jaundice.
This is why "watch and wait" — sometimes called expectant management — is often the recommendation for most patients with asymptomatic gallstones.
When is earlier surgery the better choice?
There are well-defined situations where the calculus changes and prophylactic removal of the gallbladder is recommended even in the absence of symptoms:
• Patients with diabetes, where biliary complications carry a higher mortality
• Patients with sickle cell disease or other haemolytic disorders
• Patients with very large gallstones (greater than 3 cm), which carry an increased risk of gallbladder cancer
• Patients with calcified ("porcelain") gallbladder, also linked to cancer risk
• Patients with gallbladder polyps over 10 mm coexisting with gallstones
• Patients undergoing certain bariatric procedures
• Patients on GLP-1 receptor agonist medications (Mounjaro, Wegovy, Ozempic), where rapid weight loss and altered gallbladder motility substantially increase the risk of acute biliary events
In each of these groups, the risk-benefit balance shifts toward earlier intervention.
When watchful waiting is reasonable
If you have asymptomatic gallstones, no high-risk features from the list above, and you understand the small ongoing risk of developing symptoms, expectant management is a safe and evidence-supported choice. You don't need surgery "just in case."
What watchful waiting involves in practice:
• No restriction on diet, although some patients find that limiting very fatty meals reduces the chance of triggering an episode
• Awareness of the symptoms to watch for: severe upper-right or upper-central abdominal pain, pain radiating to the right shoulder, nausea and vomiting, jaundice, or fever
• Prompt review if any of those symptoms develop
When earlier surgery is reasonable
Conversely, there are valid reasons to choose elective cholecystectomy even without high-risk features:
• Practical: planning surgery on your terms (around work, travel, family) is preferable to an emergency admission
• Geographic or lifestyle: frequent travel to areas with limited healthcare access raises the threshold for "wait and see"
• Risk aversion: some patients place high weight on eliminating future uncertainty
• Concurrent surgery: if another abdominal procedure is planned, combining can make sense
Neither approach is "right." Both are reasonable. The job of the consultation is to make the choice an informed one. If you’d like that informed discussion - with someone who will recommend surgery only when it’s genuinely needed - I’d be glad to help.
The role of GLP-1 medications
The increasing use of GLP-1 weight-loss medications has changed the landscape of asymptomatic gallstone management. Peer-reviewed evidence — including the STEP trials and a 2022 JAMA Internal Medicine meta-analysis — shows a 1.37 relative risk of biliary disease in patients on these medications. The mechanisms are rapid weight loss altering bile composition and pharmacological reduction of gallbladder motility. If you have asymptomatic gallstones and are starting or already on a GLP-1 medication, this is a specific situation where earlier surgical assessment is worthwhile. See our dedicated page on this topic: Gallstones and GLP-1 Agonists.
What the consultation involves
A typical first appointment includes:
• A focused clinical history — including any atypical or partial symptoms you may have dismissed
• Examination
• Review of your existing imaging
• Discussion of your specific risk factors
• Use of the RELAPSTONE tool to quantify your individual progression risk
• A clear summary of the options, with no pressure to proceed
If you decide on watchful waiting, we provide guidance on what to monitor and when to seek review. If you decide on surgery, the next step is a pre-operative fitness assessment and scheduling at the Wessex Nuffield Hospital.
Common questions about asymptomatic gallstones
1
My GP told me my gallstones don't need treating. Why see a surgeon?
A surgical consultation is not a recommendation for surgery. The value is an individualised risk assessment using tools and evidence not available in a ten-minute GP appointment, so you can make an informed decision about whether to wait or proceed.
Will eating differently make my gallstones go away?
2
No. Dietary change does not dissolve gallstones. Ursodeoxycholic acid (a medication) can occasionally dissolve small cholesterol stones but takes years, has a high recurrence rate, and is rarely used in modern practice.
If I'm going to need surgery eventually, why not just do it now?
3
This is the central question of asymptomatic gallstone management, and the honest answer is that only around 20% of asymptomatic patients ever need surgery. For the other 80%, "doing it now" means accepting the (small) risks of elective surgery for no clinical benefit. The RELAPSTONE tool helps clarify which group you are likely to fall into.
How long can I safely wait?
4
There is no time limit. Patients can be observed for years or decades. The decision to operate is driven by symptoms or the development of high-risk features, not by the passage of time.
5
I'm on Mounjaro / Wegovy. Should I have my gallbladder out before starting or during treatment?
This depends on whether you already have gallstones, the dose and duration of treatment, and your symptoms. The current evidence supports earlier surgical assessment for patients with pre-existing stones who are on or about to start high-dose GLP-1 therapy. We will assess this on an individual basis.
Next steps
If you have been told you have gallstones without symptoms and want a clear, unhurried surgical opinion:
If you’ve decided you’d like to proceed, or simply want to understand the operation, see our guide to private gallbladder surgery in Southampton.